Brain on Fire Disease: Anti-NMDA Receptor Encephalitis Explained
The words “brain on fire” are being widely searched, driven by public curiosity, patient stories, and popular media. It is a serious but treatable neurological disorder known as anti-NMDA receptor encephalitis, a form of autoimmune encephalitis in which the body’s immune system mistakenly attacks the brain.
Advances in neuroscience have revealed that this condition is one of the most common causes of autoimmune encephalitis, particularly in young adults. Although once considered extremely rare. Delayed diagnosis remains common due to its striking resemblance to primary psychiatric illnesses even though the awareness has improved.
This article provides a clinically sound and evidence-based explanation of the “brain on fire” condition. What are its causes, symptoms, diagnosis, treatment, recovery timeline, and long-term outcomes.
What Is the “Brain on Fire” Condition?
“Brain on fire” is a popular term and not a medical diagnosis. The term is used to describe an autoimmune disease first identified in 2005, anti-N-methyl-D-aspartate receptor (anti-NMDAR) encephalitis.
Definition:
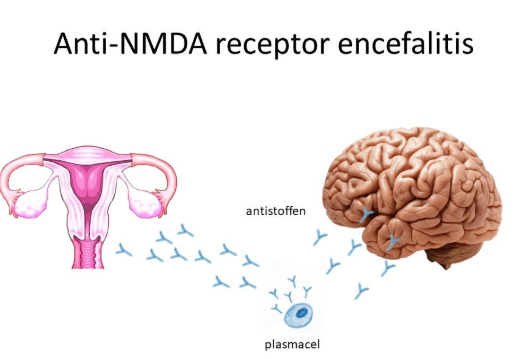
Anti-NMDA receptor encephalitis disrupts normal neurotransmission and causes brain inflammation (encephalitis) and is a condition in which antibodies target NMDA receptors in the brain. NMDA receptors are responsible for memory formation, learning, conscious thought and emotional regulation.
Brain function becomes profoundly disorganized, when these receptors are attacked.
Why Does the Immune System Attack the Brain?
Antibodies defend the body against infections, under normal conditions. In autoimmune encephalitis, treating them as foreign, antibodies mistakenly bind to brain proteins.
Known Triggers
Viral infections sometimes are the preceding symptoms.
Ovarian teratomas, particularly in young women.
Prior history of herpes simplex virus encephalitis
The cause for the majority of the cases remains unknown.
In many patients, making early recognition even more challenging, no clear trigger is identified.
Who Is Affected?
Especially women and most commonly affects young adults.
The average age of onset is late teens to early 30s.
It can occur in children and older adults.
Likely underdiagnosed and considered rare.
Early Symptoms:
Mimicking a flu-like illness, Anti-NMDAR encephalitis often starts subtly. The initial symptoms are headache, fever, fatigue and malaise. Symptoms escalate dramatically, within days to weeks.
Neuropsychiatric Symptoms:
Leading to frequent misdiagnosis, up to 60% of patients initially present with psychiatric symptoms.
Common Psychiatric Features:
Anxiety or depression
Disorganized thinking
Personality changes
Agitation or aggression
Paranoia
Delusions
Hallucinations
Many patients are first admitted to psychiatric units, because these resemble schizophrenia or bipolar disorder. Where physical illness is misattributed to mental illness, delaying life-saving treatment, this phenomenon is known as diagnostic overshadowing.
Progression: Neurological
The neurological signs emerge; and the inflammation worsens.
Neurological Symptoms
Memory loss
Seizures
Speech disturbances
Involuntary movements
Altered consciousness
Autonomic instability
Patients may experience fluctuating blood pressure, abnormal heart rate, temperature dysregulation and reduced responsiveness or coma. Intensive care is often required, at this stage.
How Is Anti-NMDA Receptor Encephalitis Diagnosed?
Diagnosis requires specialized testing and high clinical suspicion.
Diagnostic Tools
For NMDA receptor antibodies, cerebrospinal fluid (CSF) analysis.
Especially ovarian teratomas in women, tumor screening.
Blood antibody testing.
Early MRI brain may be normal.
EEG often shows diffuse slowing or epileptiform activity
Importantly, as much as up to one-third of cases may initially test negative but negative antibody tests do not exclude the disease.
Treatment: Can the Brain Recover?
Yes. Anti-NMDAR encephalitis early intervention significantly improves outcomes and is treatable.
Standard Treatment Approaches:
Followed by prolonged rehabilitation, patients often require weeks to months of therapy
Immunotherapy | Corticosteroids |
Intravenous immunoglobulin (IVIG) | |
Plasmapheresis | |
Second-line therapy | Rituximab |
Cyclophosphamide | |
Tumor removal | If present |
Seizure control | ICU Support |
Recovery Timeline: How Long Does Healing Take?
The recovery for the brain on fire is slow, staged, and non-linear.
Evidence-Based Recovery Data
In the first 6 months, rapid improvement occurs.
Up to 3 years continued recovery may extend.
Within 1–2 years, over 80% regain independent living ability.
However, recovery in this case does not always mean complete restoration.
Long-Term Cognitive and Emotional Effects
For several years after diagnosis, A 2024 study in Neurology® followed patients.
Key Findings
In at least one cognitive domain, 65% showed below-average performance.
Memory and language were the majorly affected cognitive parameters.
Beyond 3 years, 34% had persistent impairments.
Up to 30% did not return to school or work.
Academic or occupational adjustments were required for the remaining 18%.
Common long-term complaints include Brain fog, reduced processing speed, emotional dysregulation, social withdrawal and fatigue.
Why Early Diagnosis Matters
Delayed treatment increases: ICU admissions, duration of hospitalization, cognitive disability and psychosocial burden.
Before irreversible injury occurs, early recognition allows immunotherapy to halt immune-mediated damage.
“Brain on Fire” in Popular Culture
After Netflix released Brain on Fire, based on journalist Susannah Cahalan’s memoir, public awareness increased significantly.
The film accurately portrays:
Seizures and hallucinations.
Early psychiatric misdiagnosis.
The importance of specialist neurological evaluation.
Rapid neurological decline.
While it is dramatized, its clinical core is widely regarded as medically sound.
Key Takeaways:
The Anti-NMDA receptor encephalitis or popularly known “brain on fire” highlights critical gaps in healthcare.
In atypical psychosis, autoimmune causes must be considered.
Psychiatric symptoms can signal towards neurological disease
Normal MRI or EEG does not exclude encephalitis.
Awareness reduces diagnostic delays.
Multidisciplinary collaboration saves lives.
Frequently Asked Questions (FAQs)
Is “brain on fire” a real medical term?
No. It is a popular phrase referring to autoimmune encephalitis an anti-NMDA receptor encephalitis.
Can patients fully recover?
Even though subtle cognitive, emotional, social difficulties may persist, many patients recover.
Is it contagious?
No. It is not an infection but an autoimmune condition.
Is it fatal?
Delayed diagnosis increases risk, with timely treatment, survival rates are high.
Why is it often misdiagnosed?
It is misdiagnosed because the early symptoms closely resemble psychiatric disorders.
**This article is solely for educational purposes and does not provide any medical advice. Diagnosis and treatment of anti-NMDA receptor encephalitis is performed by qualified healthcare professionals.
Scientific & Medical References
- Dalmau J, et al. Lancet Neurology, 2008
- Dalmau J, Graus F. New England Journal of Medicine, 2018
- Hughes EG, et al. Journal of Neuroscience, 2010
- Titulaer MJ, et al. Lancet Neurology, 2013
- Schmitt SE, et al. Neurology, 2012
- Cognitive Revolution
- Cognitive Biases: How are we tricked to misjudge?
- Cognitive Distortions: How the Brain Tricks Itself?
- Bruner Theory of Cognitive Development
Also read more about brain and its creativity - Click Here